Every year, on 16 October, the “World Restart a Heart Day” draws global attention to resuscitation after sudden cardiac arrest. For life and health insurers, this is not “just” a medical topic. The real question is: will new rescue concepts enable more people to survive a cardiac arrest with a good prognosis? And should these survivors be assessed differently in underwriting?
The Critical Factor: Time Without Blood Flow
A cardiac arrest means the heart suddenly stops beating. From that moment on, the brain and other vital organs are no longer supplied with oxygen. Within three to five minutes, the cells of the brain begin to die irreversibly. In medical language, this period is called “no‑flow time”: the time span when no chest compressions are being performed and the body’s own circulation has not yet been restored by defibrillation. The longer this phase lasts, the lower the chances of survival. And here, literally every minute counts.1
International data show that after a cardiac arrest outside a hospital (OHCA – out-of-hospital cardiac arrest), on average only about 10% of patients are ultimately discharged alive after the subsequent in‑hospital care.2,3 By contrast, for a cardiac arrest occurring inside a hospital (IHCA – in‑hospital cardiac arrest) where professional help is immediately available and no‑flow time is typically very short, the survival rate is about twice as high, at about 20% to 25%.4,5 These figures strongly illustrate how essential a minimal no‑flow time is and how powerful immediate professional resuscitation is compared to bystander-only resuscitation.
Equally striking is the inverse approach to the numbers: for each minute of cardiac arrest without chest compression, the chance of survival drops by an astonishing 10% per minute passed.6 Against this backdrop, it becomes clear that rapid restoration of circulation is decisive for improving survival.
Progress to Date – With Limits
Precisely for these reasons, the emergency chain of response has evolved over recent decades. After an emergency call, a dispatcher-guided bystander cardiopulmonary resuscitation (CPR) until the emergency medical services (EMS) vehicle arrives at scene is now standard in nearly all dispatch facilities around the world, and the spread of automated external defibrillators (AEDs), defibrillators specifically designed for use by laypeople, has structurally improved the odds.
And yet: in many countries only a fraction of bystanders actually begin chest compression. In Germany for example, the bystander-CPR rate is about 40% to 45%, while in Scandinavian countries such as Norway or Sweden it reaches up to 70%.7,8 These differences reflect the success of long-standing public campaigns in Northern Europe, while in Central Europe and other parts of the world inhibition to act persists in the public mind.
AED use lags far behind its potential. Even in countries with dense public availability – such as the United States – AEDs are applied in fewer than 20% of eligible out-of-hospital emergency cases.9 This is a disappointing outcome, considering that early defibrillation is a key factor for better survival.
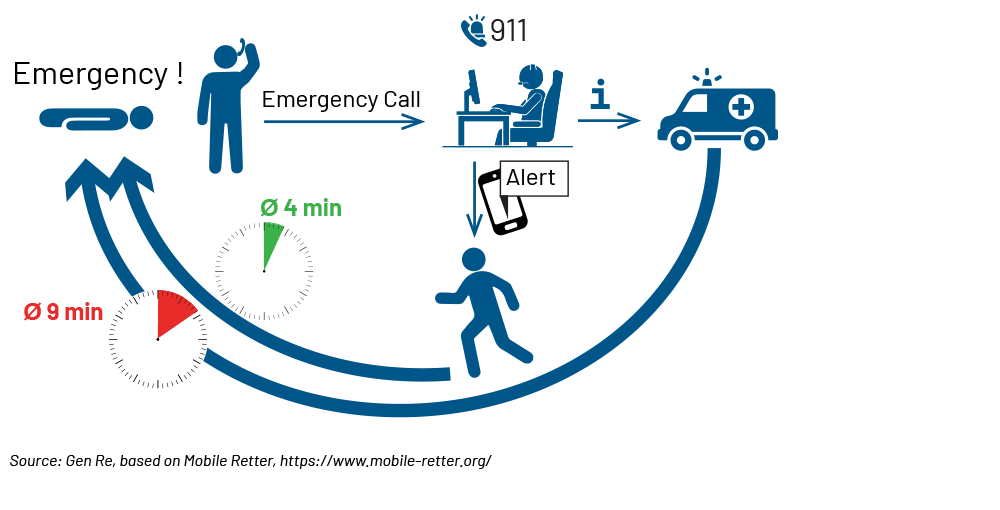
Despite concerted efforts to adapt the emergency chain of response, a lethal gap remains between the event of cardiac arrest and professional care by emergency medical services – and it is precisely this gap that the new systems addresses.
The Game-changer: Smartphone-based First Responder Systems
In a growing number of countries, medically qualified first responders – physicians, nurses, EMS professionals and in some systems laypeople specifically trained in chest compression – are alerted by smartphone app when a cardiac arrest is reported in their immediate geographic vicinity. Thanks to modern localization technology on their personal smartphones, these responders on average can reach the emergency scene significantly faster than EMS. The goal is obvious: to shorten the critical no‑flow time as much as possible.
Internationally, a growing landscape of such systems exists. In Sweden, the “SMS-Lifesaver” program was launched as early as 2012. A randomized study showed that phone-based alerting significantly increased the rate of chest compression.10 Denmark followed and established “Hjerteløber” (“heart-runner”) on a large scale, with high participation, resulting in app-alerted responders often arriving before EMS and markedly increasing the chance of early defibrillation.11
In the United Kingdom, “GoodSAM” was integrated into ambulance dispatch centers, with a focus more towards medically trained responders.12 In Switzerland, local first responder networks could document real-time gains and high feasibility of their system,13 while in the U.S., “PulsePoint” is a widespread application. Depending on the region, in addition to professional off-duty responders, CPR-trained citizens are included, so it’s a mixed system adapted to geographic challenges of the U.S. between densely populated areas and the vast countryside. Ongoing studies are evaluating its utility and implementation in North America.14
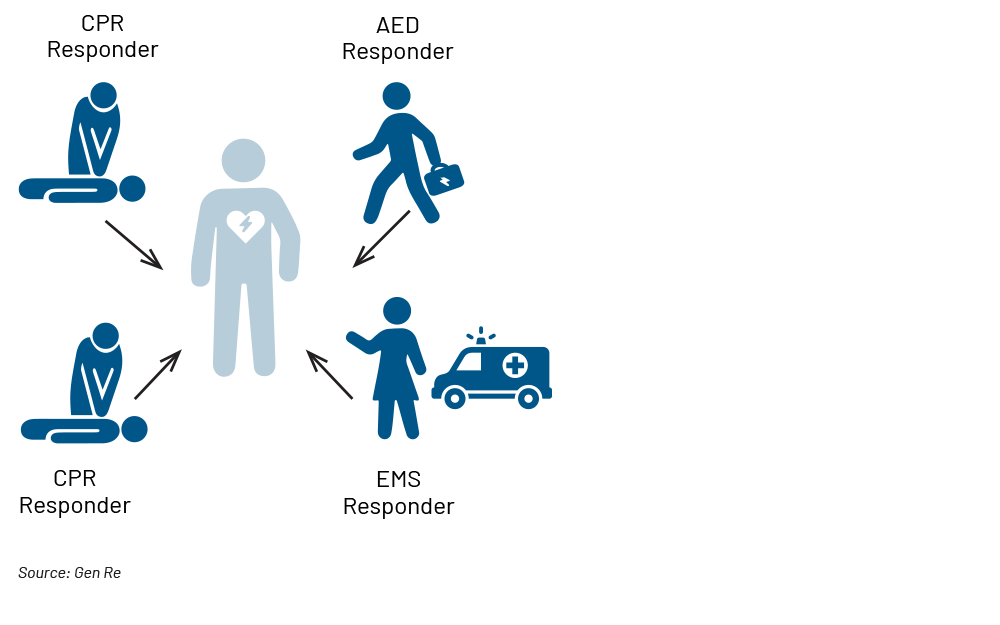
Germany is also an active market with multiple initiatives. Programs such as “Mobile Retter” (“mobile rescuers”) and “Region der Lebensretter” (“region of lifesavers”) deliberately rely on medically trained responders who are alerted by the dispatch centers in parallel with EMS. Prospective companion studies such as HEROES15 and REAP16 are under way to quantify effects on survival and neurological outcome under real-life and systemically monitored conditions. Based on early study results, the alerting algorithm was refined to further reduce time to chest compression and to increase AED use. It now alerts not only one but up to four responders simultaneously and assigns algorithm-based roles for the early resuscitation phase to each one of those.
Third-generation First Responder App With Role Assignment