- Property & Casualty
- Life & Health
- Knowledge Center
-
About Us
About Us OverviewCorporate Information
TOP

How long will I live? It’s a question that humans have pondered since the dawn of time. From palmistry to the latest health fads, we have found more or less satisfactory answers. Those of us in the Life industry, as students of mortality, are interested in a similar question: How does mortality vary and evolve by age and with time?
For a long time, actuaries have identified lower mortality with the younger and middle ages; it is only in the last three or four decades that we have appreciated the impact of mortality reduction at older ages. As we try to understand this impact, a vexing question comes to mind: Do humans have an expiry date? Implicitly, our life tables ended for many years by the ominous qω=1, everyone dies at age omega.
We have pushed ω further and further with each successive actuarial mortality table and now have disposed of it altogether, in favor of a constant, which empirically seems to be close to 0.5. Yet the question remains: Is there a maximum or will the record of 122 years held by Jeanne Calment, a French supercentenarian, stand unbeatable as it has for more than 20 years?
One way to observe what happens to the mortality for a given birth year is to look at the percentage of survivors by year until there are none. This is called the survival curve. For many years and in all developed countries, the curve has become more rectangular.
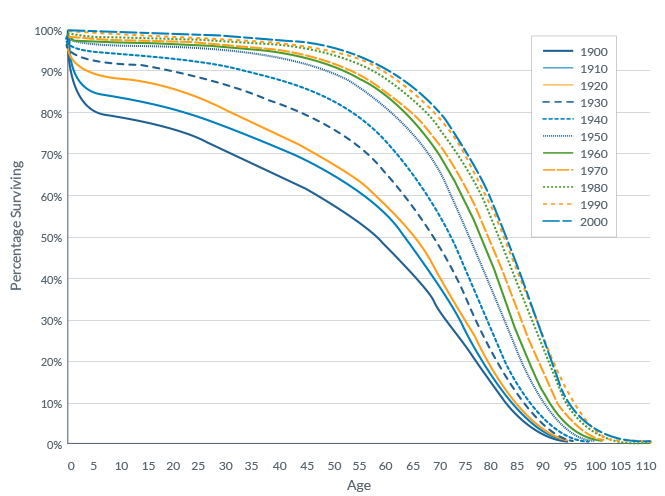
This implies that people survive to an advanced age and die rapidly thereafter. This is generally associated with what is called the compression of mortality, where deaths are concentrated around the modal age of death, the age that has the most death.
For low mortality countries (i.e., highly-developed nations), there has been some evidence of compression for several decades, depending on how you mathematically define it. The modal age of death, and the number of deaths concentrated around that age, have increased. What is more controversial is whether some populations (for instance Japanese women) are experiencing a shift to the right of the survival curve where the modal age at death has increased, but without a compression, indicating many more people reach a very advanced age and burst through the mortality “wall” instead of squashing against it. This has a very significant implication for the number of very advanced elderlies, and it implies significant population mortality improvement even at advanced ages. Results are still mixed on whether this is really happening at this time.1
Another area of controversy revolves around whether there is compression of morbidity. Will the extra years of life gained by medical progress be spent in an unhealthy disabled state? As is often the case, a good definition is key to understanding the issue. Are we talking about fewer visits to healthcare settings, feeling in better health or less disability?2 They do not necessarily move in tandem. People do not seem to be less sick but seem to be less disabled at a similar age.3
Here once again the extremely old seem to suggest special insights. Teams led by Nir Barzilai and Tom Perls, both of whom presented at past Society of Actuaries’ Living to 100 Symposiums, conducted a study comparing two populations of centenarians to their younger peers for the onset of cancer, cardiovascular disease, diabetes mellitus, hypertension, and osteoporosis. The age at which 20% of the centenarian cohorts was delayed by about two decades compared to their younger peers.4
A small study looking at a composite of health based on a combination of questionnaires, objective tests (such as the “Timed Up and Go” mobility test and the MMSE measuring cognition), as well as the ability to perform IADL (Instrumental Activity of Daily Living) had an equally amazing finding. It found that among the small group of 13 survivors now aged 96 to 106, eight were still passing the original health criteria!5
In the end, actuaries and others have two reasons to be optimistic: More people are living longer as the compression of the mortality curve, or its shift to the right, shows - and, tantalizingly, extended life is not just an addition of only unhealthy years.


















