What is anaphylactic shock?
An anaphylactic shock is the rare maximum immune reaction to an allergen, which can lead to life-threatening situations. The most common triggers of anaphylaxis include penicillin; acetylsalicylic acid; nuts; egg white; bee or wasp venom; or iodine-containing contrast media used in medical diagnostics.
The anaphylactic reaction usually manifests in varying degrees of severity within seconds to minutes after contact with the allergen. In the lowest degree of severity, there is no acute threat to life and the allergic reaction is mostly limited to the skin with redness and swelling or the formation of wheals.
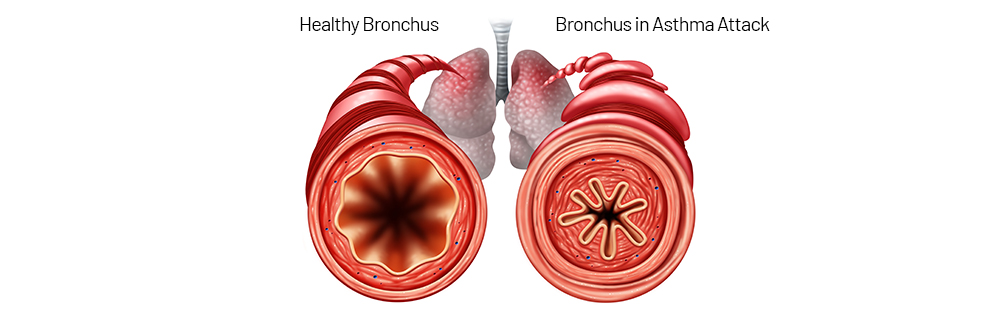
In more severe cases, the airways may swell up to a severe obstruction due to a contraction of the muscles in the bronchial tubes (bronchospasm). This can lead to acute respiratory insufficiency and an undersupply of oxygen. As a consequence, a circulatory shock may occur and lead to an acute life-threatening situation in which immediate treatment up to and including life-saving measures are required.
The lifetime prevalence of anaphylaxis is currently estimated at 0.05 to 2% in the U.S. and ~3% in Europe. Several population-specific studies have noted a rise in the incidence of anaphylactic reactions, particularly in hospitalisation rates and emergency treatment due to anaphylaxis.11 Fatal outcome is rare and constitutes less than 1% of total mortality risk in atopic people.12
Why is atopy or allergy relevant to insurance medicine?
Anyone who has the predisposition to produce antibodies against a certain substance and already has an allergy has an increased risk of developing allergic hypersensitivity to other substances in the course of life. This can occur as a result of a cross-reaction or as an independent development.
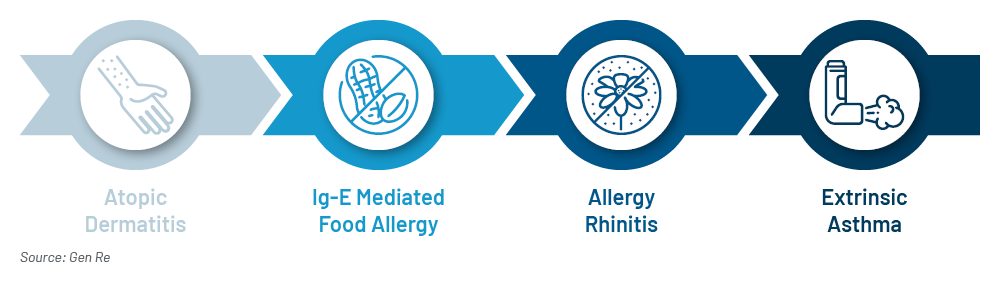
Cross-reactivity in allergic reactions occurs when the proteins in one substance (e.g. pollen) are similar to the proteins found in another substance (e.g. food). It may cause immune system reactions with symptoms to substances that contain similar substances to the already known allergen. For example, people with a birch pollen allergy are often also allergic to apples and hazelnuts.
Another medical risk is the “change of floors” of an allergy. For example, 20 to 40% of people with allergic rhinitis (hay fever) also develop allergic bronchial asthma during their lifetime.
These facts are particularly relevant in the occupational context and already in the choice of a profession. From an insurance point of view, caution is generally required in the risk assessment in the case of an existing allergy. Of course, diseases should always be assessed according to their treatability. With regard to therapy options for allergies, however, it should be noted that the first principle is allergen abstinence. Abstinence to an allergen isn’t always easy to perform, e.g. in the case of contact with allergens in the occupational environment.
Another important principle in the treatment of allergens is the control of symptoms by medication. It should be kept in mind that in the case of long-term treatment with medication, side-effects of medication may have to be expected, e.g. when taking antihistamines, glucocorticoids or immunotherapy.
Furthermore, for immunotherapy, also called hypo- or desensitisation, the actual and lasting effectiveness of the therapy has so far been proved only for a few substances (birch, hazel, grasses, alder, house dust mites, some moulds and bee/wasp venom) in clinical studies. In addition, immunotherapy is more successful with monoallergies than with multiple allergies. It is also more effective in children, adolescents and young adults than in older people.
These are the recommendations for allergy risk assessment:
- Allergies should always be considered in the medical underwriting process.
- There is significant relevance in insurability of occupational disability. For the insurability of life insurance, allergies have a significantly lower relevance, unless allergic asthma is present.
- Due to the possible development of further allergies or the danger of a change of level to asthma, an exclusion of an individual allergy or allergen won’t be sufficiently effective.
- If allergic bronchial asthma is present, the control of symptoms, measured by the frequency of attacks, is decisive.
More than 128 million people in Europe are suffering from allergies resulting in reduced quality of life. One of the top health priorities in the EU is therefore the provision of the best possible treatment and prevention of exacerbation or progression of the disease. In part 2 of this blog series Dr. Sandra Mitic talks about various treatment options and the impact on disability claims.
Endnotes
- Zuberbier T, Lotvall J, Simoens S, Subramanian SV, Church MK. Economic burden of inadequate management of allergic diseases in the European Union: a GA2LEN review. Allergy 2014; 69: 1275–1279.
- Ibid.
- Bieber T, et al. Global Allergy Forum and 3rd Davos Declaration 2015. Allergy 2016; 71(5): 588–592.
- The European Academy of Allergy and Clinical Immunology (EAACI). Advocacy manifesto. Tackling the allergy crisis in Europe – Concerted policy action needed. June 2015.
- Acevedo-Prado A, et al. Association of rhinitis with asthma prevalence and severity. Nature scientific reports 2022 12:6389. https://doi.org/10.1038/s41598-022-10448-w, last accessed, 21 June 2023.
- K. Murphy, C. Weaver. Janeway Immunologie, https://doi.org/10.1007/978-3-662-56004-4_14, last accessed, 23 June 2023.
- Bantz SK, Zhu Z, Zheng T. The Atopic March: Progression from Atopic Dermatitis to Allergic Rhinitis and Asthma. J Clin Cell Immunol. 2014 Apr; 5(2):202. doi: 10.4172/2155-9899.1000202. PMID: 25419479; PMCID: PMC4240310.
- D.A. Hill, J.M. Spergel. The Atopic March: Critical Evidence and Clinical Relevance. Ann Allergy Asthma Immunol. 2018 February; 120(2): 131–137. doi: 10.1016/j.anai.2017.10.037.
- Bantz SK, Zhu Z, Zheng T. The Atopic March: Progression from Atopic Dermatitis to Allergic Rhinitis and Asthma. J Clin Cell Immunol. 2014 Apr; 5(2):202. doi: 10.4172/2155-9899.1000202. PMID: 25419479; PMCID: PMC4240310.
- Ibid.
- Yu JE, Lin, RY. The Epidemiology of Anaphylaxis. Clin Rev Allergy Immunol. 2018 Jun; 54(3):366–374. doi: 10.1007/s12016-015-8503-x. PMID: 26357949.
- Turner PJ, Jerschow E, Umasunthar T, Lin R, Campbell DE, Boyle RJ. Fatal Anaphylaxis: Mortality Rate and Risk Factors. J Allergy Clin Immunol Pract. 2017 Sep–Oct; 5(5):1169–1178. doi: 10.1016/j.jaip.2017.06.031. PMID: 28888247; PMCID: PMC5589409.